


Why is everybody sick all the time?
Working through my anger and sadness at a botched pandemic response

Over the last two weeks I’ve written about community and how I can use what I’ve learned about apologies to strengthen my communities, especially when there are disagreements.


Having tough conversations are hard, but they are worth it1. I have a saying that I’ve become known for in some circles – “It sucks, but it’s good, but it sucks”. I first came up with this when I was learning how to feel all the uncomfortable emotions I had buried deep within me. It sucks to feel them, but it’s good to release them, but it really sucks to feel them. It’s exhausting and sometimes terrifying, especially when I share uncomfortable emotions with others.
That’s how I’m feeling this week as I struggle to write this newsletter. I’m going to write about the anger and sadness I feel, mostly at my governments, but sometimes with individuals, for how they have handled/didn’t handle the pandemic that we are still in. I need to write about it for myself to release these feelings I have. But I’m going to be honest and say that I also hope that by reading about my experiences and my anger, that you will join me with some outrage of your own after learning what has most likely been kept from you. Because the situation is bad for all of us and it needs to change.

I’m ending on a hopeful note, so I do hope you will stick with me till the end. I know that COVID and the pandemic is traumatizing for many of us, even those who aren’t experiencing long term illness. I don’t say that lightly; I am diagnosed with PTSD due to a sexual assault and I take the diagnosis seriously. But the world changed in a dangerous way and we haven’t been equipped to deal with it. This, in my opinion, has lead to many traumatized people. On top of the pandemic, there is climate change, multiple wars, and precarious political situations in most countries. I fully understand the desire to look away because it is overwhelming. So, if you have overwhelming feelings when it comes to the pandemic, I hope you will put yourself in a safe place before reading this. Curl up on the couch, make a cup of tea, listen to a grounding meditation – whatever is right for you. Because when I list what I’m angry and sad about, you might feel angry and you might feel guilty, depending on how much you know. I don’t want you to feel attacked and I don’t want you to shut down. But if you do feel guilty reading my account, I am asking you to sit with those feelings and think about how good it might feel to make some changes so that you are living more aligned with your own values. Because change is possible, and I want all of us to feel loved and accepted. We all deserve that.
Most of my anger these days is related to the fact that I have long COVID and it didn’t have to be that way. I’m also angry because millions more will develop long COVID if we stay on the current trajectory, and that breaks my heart into millions of shards of rage. Governments have the knowledge and resources to provide us protection from airborne viruses, but in too many cases, they aren’t protecting us. It makes my blood boil because I don’t want anyone else to experience the hell I’ve been living through for the past 956 days and counting, but until these protections are put in place, many will join me, including some of you reading this.
The situation when I got infected
It was December 2021, and I was working as a bartender for a Toronto brewery, a job that held the promise of future event management work, which was my career before the pandemic began. I was at a point in my life where I was so happy and feeling so healthy. In fact, I was in the process of weaning off the antidepressants I had been taking because my doctor and I agreed I didn’t need them anymore. My ex and I had just moved into a new apartment together, so I was no longer living in his apartment, now it was our apartment. I was optimistic about my future and that felt so good.2
At work I wore a blue surgical mask as required. The provincial vaccine mandates were in place and we scanned customers’ QR codes before allowing them to stay, which meant that everyone unmasked had received at least their initial vaccines. Although we were sold a story that being vaccinated would allow us to live “normally” without fearing infection or reinfection, that story was clearly untrue, even 3 years ago. My friends and I who worked in hospitality braced for our inevitable infections. What could we do when our jobs put us in harm’s way? This was our new reality, but at least with our relative youth and health, we told ourselves, we would only be sick and out of work for 10 days. Maybe you can relate to those thoughts.
There was pressure for bars and restaurants to be closed as this first Omicron wave surged up. Our provincial government made the curious decision at first not to shut them down, but to force us to close the doors at 10pm, as if the virus was safe during the day. Many bars in the city proactively closed the week before Christmas “out of an abundance of caution”, although I later heard it was actually because so many of their staff had become infected that they didn’t have the employees to stay open.
One of regulars was very anxious about the proposed lockdown because she lived alone and our bar was her main place to be social. She worried about her mental health and what would happen if she couldn’t socialize with us. Hearing that made me feel like we were providing an essential service and I was really proud to be a part of it. I wasn’t “just” a bartender. I was needed and an essential part of the community.
Then I got infected and everything changed.
The lockdown did happen for the month of January, but I didn’t get better in that time. During one particularly bad coughing fit, I vomited into the bathroom sink before falling onto the floor, sure I was about to die. Other than my manager asking when I would be coming back to work, I didn’t hear from any colleagues. I sometimes wonder if that regular ever asked why she never saw me again or if she wondered about my mental health at all, which deteriorated quite a bit, a common result after SARS-CoV-2 infections. But maybe she got infected and depressed too. Is it irony if the place you think will keep you healthy turns out to be the place most likely to make you sick?
I looked online for information on how long I might expect to be sick. I read that most people recover within 3 months, which would be just after my 37th birthday. I counted down the days and figured I could deal with the pain and misery until then. I joined a long COVID research study and tried to exercise my lungs by blowing up balloons and my mind by taking an online accounting course. If only I knew then how damaging those good intentioned actions could be, but my public health units didn’t have warnings about long COVID. Other than AIDS, post-infectious illnesses predominantly happen in women and have not been taken seriously, so while I am very angry and sad that our governments, public health, and health care systems did not jump up immediately to learn all they could to warn us what might happen, I am not surprised. It’s easier to blame us as being hysterical, depressed, anxious, and/or fat than take any responsibility for our health.
My birthday came and went, but I did not improve. I joined long haulers Facebook groups and searched for more answers. This is when I developed a white-hot fury that lasted for years because SO MUCH WAS ALREADY KNOWN IN DECEMBER 2021. I was horrified to see that there were researchers, clinicians, and patients who had been sharing information that could save lives and prevent disability, but their messages were routinely dismissed or even mocked. I could have learned from them and saved myself, but governments seemingly decided that short-term economic gains were more important than providing us the truth and following the precautionary principle. They didn’t want us to panic and reassured us that as long as we were vaccinated, only the elderly and those already sick were at risk of death or prolonged illness. Setting aside how distasteful, to put it politely, it is to convince us not to worry about the safety of the members of our community who are undeniably at risk, it was abundantly clear that even the young and healthy were becoming disabled! And it was also abundantly clear that we had the technology and tools to prevent infections in a way that vaccines can’t.
Friends and family members sent me news articles suggesting that my Omicron infection would protect me for life so I should not worry. I felt like I was living in The Twilight Zone because the actual research suggested not only could I be reinfected with future mutations, but there was a good chance the virus was silently wreaking havoc on my immune system, blood vessel walls, brain, and nervous system. The respiratory issues were the least of my problems.
I read this article about the history of the aerosol vs droplet debate. “Oh my God”, I thought. “The WHO were warned by experts in April 2020 that the virus likely spread by aerosols and they didn’t tell us this was a possibility. They did the opposite, in fact and doubled down that it spread by droplets only. Why couldn’t they open their mind to this possibility?!? But at least I can warn others now. I can explain to my friends and family and protect them”.
I found this video that wonderfully explains the physics of respirators, such as N95s, and why they are superior to surgical masks. I immediately stockpiled N95s for me and my ex to give us the best protection going forward. This video, by the way, was published to YouTube on June 18th, 2020. I am so angry I didn’t see it sooner.
Why had it not been promoted by public health and every news station? Why were hospitals and medical facilities insisting on surgical masks? Why were our lives and health being sacrificed? Why weren’t those in charge listening to the people trying to protect us? Why are they still not giving us the correct advice so that we can protect ourselves and others?
For the most part, my friends and family did not listen to me and that hurt. I frequently cried to my ex, saying I would feel responsible if any of our relatives got sick and died because I couldn’t convince them to protect themselves. We both suspected his mom’s COVID infection sped up her cancer progression and death. I sometimes wonder if the reason he can’t bear to speak with me anymore is because I failed to convince her. I hate that I couldn’t convince her because my precautions were viewed as over-the-top compared to what she was being told by her doctors. Who was I to say I knew better than her doctors? Even when she was being treated in the world-class cancer hospital, a place full of vulnerable patients, the standard was a surgical mask. I was so angry. And I was angry at my ex for not demanding that her nurses and doctors wear respirators around her. But that responsibility shouldn’t have been on him, especially during that stressful time. The science had been settled since before SARS 1: respirators are what to wear during respiratory illness season.3
What did we learn from SARS 1 in Toronto and Vancouver?
The documents that haunt me the most are the reports commissioned by the Ontario and Canadian governments after the first SARS pandemic. Why did the WHO need more data about aerosol transmission when this section4 of the Ontario report exists, in which it compares Toronto/Scarborough Grace Hospital’s response unfavourably to Vancouver/Vancouver General Hospital’s response:
Dr. Elizabeth Bryce, head of Infection Control at Vancouver General Hospital, said:
Respiratory precautions meant the use of an N95 respirator until the clinical condition was clearer.
N95 respirators were not standard respiratory protection at the Grace, and were not used by staff who treated Mr. T.
This was a significant systemic advantage for Vancouver General. Its emergency department staff were already protected by the kinds of respirators that would not become standard protective equipment in Ontario until weeks later. The ICU at Vancouver General had used N95 respirators for a few years. Fortuitously, the emergency department also began using them some months before SARS hit.
N95s didn’t used to be controversial! I am so upset that this amazing tool that can keep us safe from viruses, but also wildfire smoke, cigarette smoke, pollen, dust, and other allergens, has been demonized rather than normalized - even in hospitals!!! What. The. Actual. Fuck.
In the Canadian report5, it discusses what happened during a lull between the waves, called SARS I and SARS II:
The Provincial Operations Centre was dismantled. The physician-in-chief of a major teaching hospital later observed that there was "a great and understandable rush to make things normal again after SARS I."
By mid-May, all levels of government were presenting a unified picture to the public that SARS had been contained. Rather than presenting data about the cumulative number of people labelled with probable or suspect SARS, health officials began to highlight the declining number of "active" cases and the number of new cases - figures that were not only more reflective of disease activity but also less dramatic. Health Canada began to issue bulletins only weekly, and reported in its May 21, 2003 update that no Canadian had experienced the onset of symptoms for over a month.
It appeared that the total number of cases had reached a plateau - 140 probable and 178 suspect infections. Twenty-four Canadians had died, all in Ontario.
And from section 2G, discussing the second wave that led to more deaths and long-term illness:
"SARS I was not avoidable. We were struck by lightning. Everything after that was." - Dr. Richard Schabas, Chief of Staff, York Central Hospital.
“Everything after that was [avoidable]”. In my mind, that includes most of the devastation of COVID-19, especially in Canada where we could have learned from our past mistakes but didn’t. We’re making the same mistakes again, even down to reducing communications of valuable metrics, except this time there are thousands of people still dying. I’ve spent so much time awash in despair, knowing my life could look very different right now if my governments, both current and past, had prioritized implementing the lessons from SARS 1. Sometimes that despair is more unbearable than the illness itself. I mean, what is the point in me trying to live when I’ve been failed, and continue to be failed, by so many people? I want to see the Sliding Doors movie of my life in which I’m shown me living in a Toronto with a proactive pandemic response, alongside my actual life with the current reactive governments.
But that can only be a dream. Instead, I like to think of myself as a version of Batman because I will not fall victim to despair. Can I figure out a way to turn my pain into a warning to protect you and your loved ones? My workplace failed to keep me safe. But can’t we change things so yours protects you?
I’ve looked to history a little bit to see if I can find comfort. I wouldn’t say I’ve found comfort, but it has helped me strengthen my resolve to stay the course because eventually we humans do figure it out. Did you know that one of the first people to recognize the importance of handwashing to reduce infection, Ignaz Semmelweis, was hated by his fellow doctors for this discovery and his advice ignored? Or, that it took 17 years from the time John Snow, the man who realized unclean water was the source of cholera, published his first paper to be believed? In Ontario, smoking wasn’t banned inside public spaces and workplaces, including bard and restaurants until 2006. That is approximately 70 years after the first case reports linking cigarette smoking to lung cancer. As a species, it seems humans need a lot of prodding to adapt to new knowledge, so, it shouldn’t be a surprise that the same is happening now.
I hear many excuses as to why we shouldn’t act on current research: the study was too small, or if it was big enough it was in veterans, so not applicable to the general population. That study was in unvaccinated people so no longer relevant. That one was in vaccinated people, so everything bad is because of the vaccines. Those bad results were in people who were hospitalized. Those brain scans are from primates, but not human primates. That research is from two years ago - I’m sure it’s better now. That study relied on self-reporting so it can’t be accurate. That study was from a different country, so it doesn’t apply to me. Individually, each skeptical response might be valid. But when you put everything together, the situation becomes clear: SARS-CoV-2 is a virus everyone should avoid as much as possible.
My hope is that by contributing my story, I will help to speed along the process to the point where the majority of people see our reality for what it is. I want to minimize the number of people who die and are disabled from a preventable disease and speed up the timeline for finding treatments and a cure.
So, what can we do?
Masking forever, everywhere, all the time, isn’t my end goal and I don’t think it’s what anyone wants. In the analogy to clean water, masking is like a boil water advisory. I think everyone who lives in municipalities that clean our water is grateful for this service, right? I know I am. I likewise think it should be the government’s responsibility to clean the indoor air we breathe and enact legislation that requires non-government buildings to supply safe air, similar to the Smoke-Free Ontario Act. I’m grateful that restaurants don’t allow smoking anymore and I would be thrilled to eat in them again when their air is cleaned.
I’m confident it’s a matter of when we will clean all indoor air, not if we will, as it is the logical investment to make for a healthier population and therefore a healthier workforce and economy. We can put pressure on our politicians to act now rather than later. You are free to use any of my words in this article to form your argument or share the whole thing directly.
Not yet convinced? A study was published recently that compared infection rates between the A/B Wings and the C Wing of a long-term care facility in Edmonton.

ASHRAE is “a global society advancing human well-being through sustainable technology for the built environment”. Their 170 Standard recommends two air exchanges per hour (ACH), which means that every hour the entire amount of air in the space is replaced with new and/or recirculated air twice. The CSA Z317.2:19 Standard requires 4 ACH, of which 2 must be outdoor air. The 241 Standard was designed for healthcare resident rooms, but it is appropriate for any space where it is reasonable to expect humans with respiratory infections to gather, such as schools, workplaces, restaurants, prisons, and event spaces. It is harder to compare this Standard to the previous two as it measures the volume of air in cubic feet for each minute it moves (CFM) per occupant. Since humans breathing can be a source of infection, it makes sense to have a system that will clean the exhaled air quickly, before it can be inhaled by someone else. The 241 Standard is 50CFM/occupant. (To learn more about cleaning indoor air from an HVAC Engineer, this is a good site to bookmark and refer to).
As you can see from the study’s chart, the C Wing had a higher percentage of rooms compliant with all three standards, as well as markedly fewer infections. Cleaning the air works! This can be done with the building’s HVAC system, Far-UVC, portable air purifiers, and opening doors and windows6.
If you can afford to, clean the air you breathe in your home, vehicle, workplace, and everywhere else you spend time. And share the good news that we aren’t helpless to this virus! We can take control. This site independently tests and reviews air purifiers and I recommend checking it out to make an informed decision on which product will best serve your needs. You could also ask your local schools and daycares if they have upgraded to the ASHRAE 241 Standard, and why they haven’t, if not. Help them achieve this goal either through advocacy and/or buying them air purifiers. We owe our children this safety; our future may depend on it.
But isn’t it just a cold now?
I really wish it were just a cold now. I wish those of us, like me, who got infected during the first Omicron wave were the last to experience long term-damage from the Sars-CoV-2 virus, but that sadly isn’t the case. Deaths are still excessive compared to pre-pandemic levels and disability is skyrocketing.
This discussion about how the American life insurance industry is viewing the data on deaths and disability is sobering and illuminating. From February 2018 to February 2020, excess deaths hovered around 0%. As expected, they shot up in 2020, reaching as high as 40% some months. In 2022, well into the Omicron era and a time with much of the population vaccinated, excess deaths dropped, but were still over 10% for many months. In 2023 the average was 6%. This seems encouraging, as the line is trending down. But it is actually concerning, because at no point since the pandemic began has there been a month with negative excess mortality. Death from COVID was expected in the vulnerable, but if the emergency was truly over, there should be a valley of negative deaths after the mountains of excess deaths, because we only die once, right? With so many extra people dying in 2020 and 2021, we would expect fewer deaths in 2022 and 2023 because those people were not dying in the latter years from cancer and heart attacks, for example. But there has been no valley. COVID is still directly causing deaths at all ages, but also more than likely indirectly causing deaths as it damages all parts of the body that are connected to blood vessels, which is to say, the entire body. Strokes and heart attacks, for example, can be versions of long COVID. Infections are turning us into the vulnerable. You are still at risk of dying from COVID.
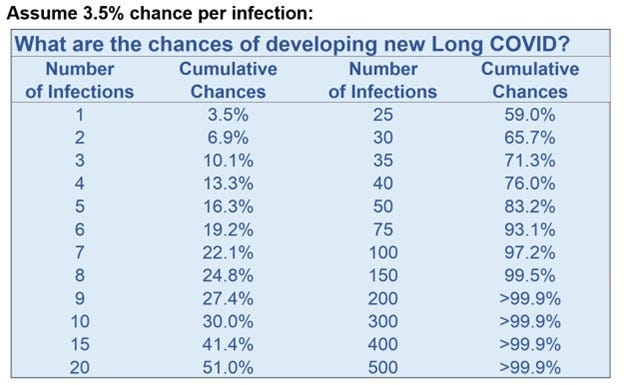
Another study recently came out that showed the incidence of getting long COVID from Omicron was 7.76% in the unvaccinated and 3.5% in the vaccinated, compared to 10.42% for pre-Delta. This was read by many as good news and a reason not to panic. And while I agree there’s no need to panic, I do think that a 3.5% chance of getting a long-term illness is high enough to do everything you can to avoid it, especially when you do the math for the cumulative risk with reinfections as Dr. Mike Hoerger did in a recent Twitter/X thread. Here is what that looks like:
Now, you may be thinking to yourself that outside of avoiding viruses, you take care of your health through diet and exercise and therefore don’t need to worry about this virus that has, to date, perhaps just given you sniffles and a sore throat. I sincerely hope you are correct! And there was a small study that showed some people do have a gene that seems to protect them from infection, so there is a chance you will never personally be impacted by this virus.
But.
Think back to what I wrote last week and consider the web of people you rely on in your day-to-day life. Now imagine what your life will be like if 6% more people than expected die each year. Then imagine what might happen if more than 20% of them develop long term health issues after 6 infections. Maybe you’ve already been disappointed because of cancelled concerts or your favourite athletes unable to compete in the Olympics or Tour de France. Imagine what will happen if our children grow up, but can’t enjoy life, can’t work, and can’t pay enough taxes to fund all the services we rely on because we didn’t want to make the investment to keep them safe. This is a crude and selfish way of looking at people, but we need to be practical as well as compassionate. When my parents grumble about my demands to keep us safe, I hope they are thinking about how they are going to need me to be as healthy as possible in the future as they have no other family nearby to help care for them as they age.
Think about how overcrowded hospitals are already, and then try to imagine what it will be like in a decade - 15 years after the start of the pandemic - if the average person gets infected every year. Already we’re seeing cracks in the systems as school and work attendance have plummeted. I had a nine month wait to see my cardiologist and I’m in the middle of a two year wait to see an immunologist! Our healthcare reality isn’t great! Now think back to 2020 and what you expected life would be like when we went back to “normal”. Did it include so much sickness? Is this the present and future you want?
It’s not what I want. I don’t want you to learn the hard way how lonely and devastating it is to live with long COVID. I desperately want you to learn from my experience so you will do what you can to trap viruses in purifiers rather than let them infect lungs. For me personally, I want a future where I get to regularly see friends and family in person because the air everywhere is cleaned and I don’t have to worry about their exhaled breath infecting me. I want researchers to stay healthy to create treatments and a cure so I can get better. The current world, where they are, and I am, consistently at risk of reinfection makes that future unlikely.
Which brings me to the uncomfortable subject of asking you to mask
Until our governments and building owners make all the necessary investments to clean indoor air, we must protect ourselves with respirators. I hope, after reading everything I’ve written7, you agree that we need to protect each other8. I can accept if you don’t like what I’ve written and would prefer to ignore this reality. I think of our situation like the scene in the Barbie movie where she’s given the “choice” between the high heels and Birkenstocks: she wants the high heels but must choose the sandals.
I know it can be difficult to stand out from the crowd by wearing a mask. Until masking is normalized again, you will probably get stares and possibly negative comments from others. I am asking you to do something that is hard and uncomfortable, and I am sorry that it isn’t easier; in my experience it gets easier with practice. Please know that I have so much gratitude for you every time you wear a mask. You will never know how much death and disability you prevent by wearing a mask, but that is what you are doing: (mostly) thankless hero work.
One-way masking, where I wear my N95 in places where others don’t mask at all, does a lot to keep me safer, so you might think that’s enough for those of us who want to protect ourselves. That we have the tools for “you do you” public health to be enough. But not everyone can wear a mask - think toddlers, babies, and some disabled people, so we need to mask to protect them. Others can’t afford high quality respirators, so we must mask to protect them as well. Symptomatic sick people often don’t wear masks because the stigma is too high. We need to make it easy for them to mask. We need to participate in community care and destigmatize masking for everyone.
If the idea of masking in public fills you with dread, I have compassion and empathy for you. I know how hard it is to do something I don’t want to do, even if I know it’s the right thing to do, and I imagine masking is a similar situation for many. Here are some suggestions for how to work up your courage to mask in public:
Practice wearing it at home to get used to the fit and how it feels
Bring it with you when you go out, in case you are in a situation where you want to wear it
Thank the people you see wearing masks and tell them you are working on building up your courage to mask too
Wear a mask when you see someone else masking as you won’t be the only one
Talk about this article with a friend or family member and go out in masks together
Search the hashtags #YallMasking and #SaltingTheVibe on social media to see proof that you aren’t alone
Donate to a mask bloc like https://www.evidencebased.ca/donate-mask/ so that people who can’t afford masks can get them for free
Tell your hospitals and medical facilities you would feel safer if they required staff and patients to mask
Tell your politicians you will not vote for them if they support mask bans
Remember, it just takes a few brave people to start a movement!
There is more I could write, and likely eventually will write on this topic. I’m sure other long haulers would focus on other studies or priorities, but I’m satisfied with what I’ve written as a medium-length overview9. I’m not turning this newsletter into a COVID newsletter, but I do have more anger to work through and I want to find out if I can find forgiveness for those who fail to protect me. I thank you for reading to the end and once again, I thank everyone for every contribution you make for a safer future.
Most of the time. Sometimes people don’t listen in good faith and no convincing argument will change their mind. It might be better to save one’s energy and not have the hard conversation with someone like that. Other people react with violence to ideas they don’t like, so it might not be worth talking with them either.
I was, as you will know if you’ve read this newsletter:

I was not giving myself a lot of self-love or compassion. But within that context, I was feeling better than I had in ages.
which, until we make changes, is year-round now.
Volume 2, Spring of Fear, Chapter Three: The Story of SARS, Vancouver: A Tale of Two Cities
Chapter 2 – SARS in Canada: Anatomy of an Outbreak, section 2F
Unless the outdoor air is strongly polluted and/or full of wildfire smoke.
and double-checking the links I’ve provided if you don’t trust me
If you don’t agree with me, I’m interested in hearing where you think my argument falls apart.
Of course, let me know if my facts are incorrect though
You may wish to look into the work of Rebecca Tolin (both her website and Youtube channel). She is currently a mind-body coach who overcame 13 years of CFS/ME and has worked on studies using these methods to treat long-COVID and also helped others with her courses (self-guided and live). I think her approach meshes well with your work processing your feelings about life and relationships with others.